
In the first place, diagnostic tests for low back pain can be quite challenging to the physician who wants to diagnose the exact cause of lower back pain. With this in mind, as mentioned above, pain and a decreased range of motion are the obvious initial findings. For one thing, the physician will check the patellar reflex and the ankle jerk reflex as a weak tendon reflex at the knee would point to a L3 or L4 nerve root compression.
Missing tendon reflexes
On the other hand a missing ankle tendon reflex would be pointing to a S1 nerve root compression and would be associated with a drop foot. In the presence of such signs (maybe only in 3 to 5 % of all acute lower back pain cases) the physician orders a CT scan or MRI scan to rule out a disc herniation. Often there might be an acute change in the first few days and then the irradiating pain into the leg would retreat and stay above the knee level.
Reactivation when tendon reflexes recover
This usually is a good sign and often no further testing is required, just reactivation. Often no testing other than observation by the physician has to be done up to 6 weeks into the acute back pain. As 90% of patients with acute lower back pain will have recovered within this period of time, much unnecessary testing and X-rays can be avoided. However, if symptoms persist, the physician has a number of options.
X-ray tests
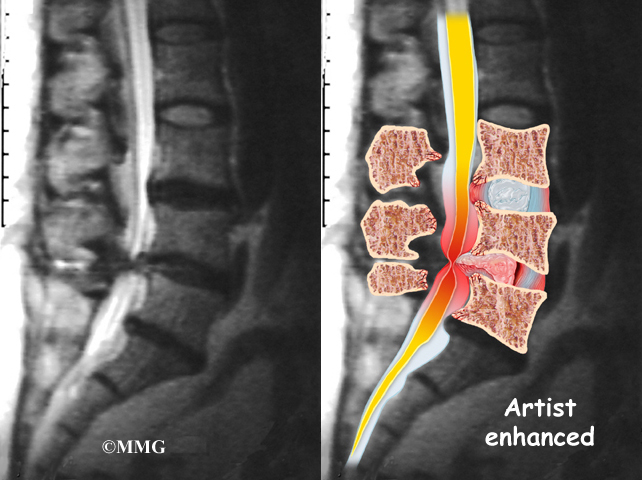
When the physician suspects osteoporosis and a compression fracture, he orders plain X-rays, which usually show the compression fracture. Degenerative changes in the spine show well on plain X-rays as well. However, the X-rays cannot distinguish between old or new compression fractures. A bone scan will show active uptake in a compression fracture that this is new. An old compression fracture would not show uptake on the bone scan.
Bone scan as a screening tool
The bone scan is also good as a screening method for bone metastases, but also for arthritis of facet joints. The radiologist can depict this well (e.g.spondyloarthropathies and degenerative arthritis). In sciatic pain, as mentioned above a CT or MRI scan should be ordered. These tests show the details of the relationship between the nerve roots, the bony structures and the discs. This way disc herniations, infections of discs (discitis) and nerve root compressions can be visualized. Degenerative changes of the discs show up really well on the MRI scan as desiccation (loss of normal water content).
Further tests for spinal stenosis
If a spinal stenosis is seen on an MRI scan , but the physician is not entirely sure about the extent of this or the effect on the nerve roots in terms of compression at possibly several levels, a myelogram can be done. Here the radiologist injects contrast dye, a radio-opaque material, into the subarachnoic space (inside the sac where the nerve roots go through) and more details can be seen, particularly, if this is combined with a CT scan. This test is called “post myelogram CT scan”. A neurosurgeon likely will want to have these tests done before a surgical procedure would ever be contemplated, so the surgeon knows exactly what to expect before the surgery is being done.
Blood tests
Appropriate blood tests would possibly be done as well depending on what condition the physician is looking for. This would include HLA B-27 to rule ankylosing spondylitis, RA titers to rule out rheumatoid arthritis or ANA titers to rule out lupus.

Diagnostic Tests For Low Back Pain
Here is a table that summarizes the more common causes for lower back pain.
Common causes of lower back pain
| Cause or disease: | Comments: |
| lower back strain | may cause 80% of back pain |
| facet joint disease | common in older patients |
| spondyloarthropathies | ankylosing spondylitis, psoriasis, ulcerative colitis, Crohn’s disease |
| osteoporosis | associated with compression fractures |
| scoliosis | congenital S-shape curve of spine |
| spinal stenosis | congenitally narrow spinal canal or acquired from degenerative changes |
| posttraumatic fibromyalgia | often following MVA’s |
| disc herniation with or without sciatica | 3% or less, needs surgery |
| spondylolisthesis and other congenital malformations | 1 to 3 % of lower back pains |
| bone metastases | commonly from prostate, breast, colorectal, uterine, cervical or ovarian cancer |
| rheumatic illnesses | rheumatoid arthritis, lupus, ankylosing spondylitis |
References
1. ABC of rheumatology, second edition, edited by Michael L. Snaith , M.D., BMJ Books, 1999.
2. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 52.
3. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 275,p.2429.
4. HA King Orthop Clin North Am 1988 Apr;19(2):247-255.
5. HA King Orthop Clin North Am 1999 Jul;30(3):467-474, ix.
6. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 59.
7. JA Smith Orthop Clin North Am Jul 1999; 30(3): 487-499.
8. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 56, p. 469.
9. Wheeless’ Textbook of Orthopaedics: http://www.wheelessonline.com/ortho/arthritis
10. Goldman: Cecil Textbook of Medicine, 21st ed.(©2000)W.B.Saunders
11. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
12. Rakel: Conn’s Current Therapy 2004, 56th ed., Copyright © 2004 Elsevier





{kind=link}