
Introduction
First of all, bladder infection (medical term: cystitis) is notably one of the most common forms of urinary tract infection in women. The urethra in women is short in comparison to the male urethra. For this reason bacteria find it much easier in women to invade the bladder in a retrograde fashion. Furthermore, another reason is that hormone changes with pregnancy lead to less peristaltic activity of the ureter, the bladder and the urethra. The end result is that infections in the bladder happen easier during pregnancy and happen more often in non-pregnant women than in men.
Bladder infection symptoms
Infection of the bladder, or “cystitis” in medical terms, almost always happens suddenly. The urine production is changed in that there is painful and frequent urination of small amounts (polyuria). Consequently, there is an urgency to urinate even when the bladder is empty. This is as a result to the irritation of the bladder wall from the inflammatory process. Bladder spasms can develop due to that. Likewise there can be back pain and a pain above the lower pelvic bone (suprapubic pain). The patient often has to get up several times during the night to urinate. In about 1/3 of the patients the urine will have blood in it and all of the patients’ urine will show a degree of cloudiness (opaqueness). In contrast, in older patients, particularly a nursing home population, cystitis can be asymptomatic (Ref. 1, p.1889).
Diagnostic tests
First, the health professional examines a urine sample first with a diagnostic test stick to indicate whether or not white blood cells, blood or E.coli bacteria are present in the urine. Second, the lab technician decides whether to do a more thorough examination with microscopy. This involves staining bacteria and white blood cells and studying them in more detail. Usually lab tests for culture and sensitivity testing of urine is necessary as well. This takes two days.
In the meantime the physician will come to a clinical diagnosis based on the preliminary tests, even before the culture and sensitivity testing comes back. If there is anything more going on than a simple bladder infection, the physician may want to refer the patient to a urologist to do further investigations such as a cystoscopy (looking into the bladder with a fiberoptic instrument). This would reveal such things like benign bladder polyps, cancer of the bladder, chronic vesicoureteral reflux etc.
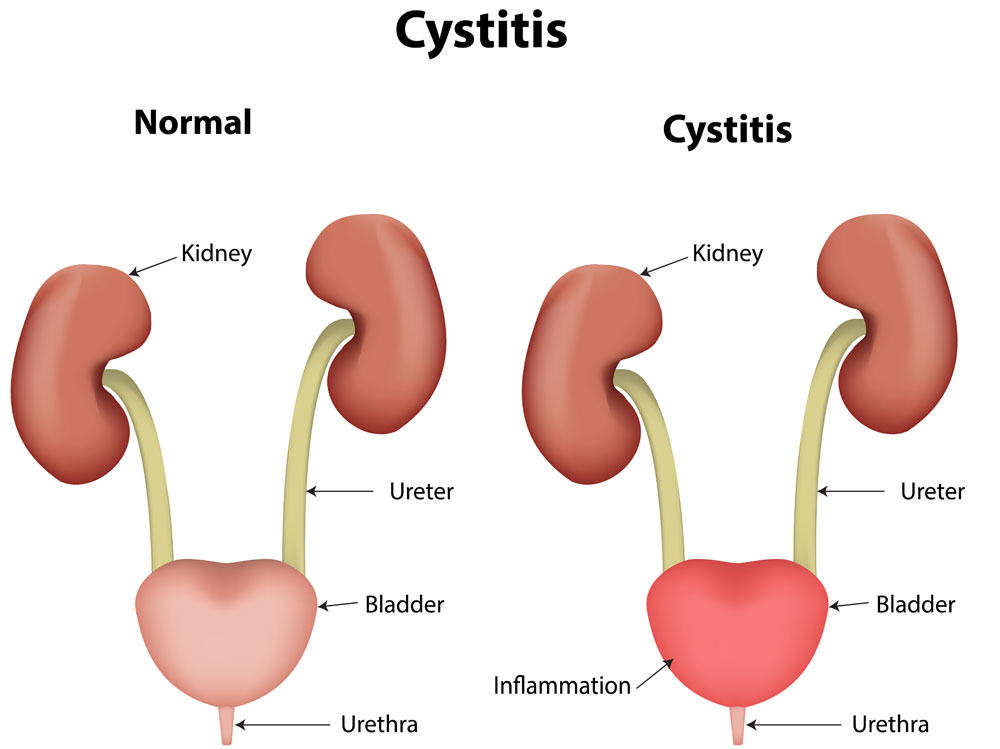
Cystitis (Bladder infection)
Treatment
We know from follow-up studies that not every patient is compliant and takes the medicine that the physician prescribed. Certainly, some of these patient did not take their antibiotic. We know that some of these patients probably cured their bladder infection with increased fluid intake only. However, others got a cystitis, which was more more chronic and more difficult to eradicate. At the present time the generally accepted rule is that the physician treat a simple bladder infection (cystitis) with a 3 day course of trimethoprim-sulfamethoxazole.
In men the caregiver treats with this antibiotic for 10 days as bladder infections are otherwise recurring frequently. If a patient had recently a prior bout of bladder infection, the antibiotic treatment time is 14 days in an attempt to eradicate the infection. The urine of people with diabetes often has sugar in it. Hence, physicians like to treat diabetics longer with antibiotics. Sugar is a growth medium for bacteria. In diabetics antibiotic therapy takes longer to eradicate the infection.
Chronic recurrent bladder infections
If following this there is still a recurrent infection, a urologist should investigate this patient. The underlying cause needs to be treated by the specialist. If resistant strains are found, the antibiotic may have to be switched around.
In nursing home patients where patients are more sessile and urinary retention is more common, recurrent bladder infections are common place. However, in this special subpopulation there is often a lack of fluid intake and it is a danger to overtreat this patient group. Increased fluid intake, more activity, cranberry juice are all simple measures that should be utilized. Sometimes there is a resistant strain found in a urine culture. If the patient has no clinical sign of bladder infection, the physician may elect to observe. The physician may repeat the culture a few days or weeks later, provided the patient is stable (Ref.1, p.1890).
References
These are a few references that describe urinary tract infections in more detail.
1.The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 227.
2.The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 261.
3.The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 164.
4.James Chin et al., Editors: Control of Communicable Diseases Manual, 17th edition, 2000, American Public Health Association.
5. David Heymann, MD, Editor: Control of Communicable Diseases Manual, 18th Edition, 2004, American Public Health Association.
6. Suzanne Somers: “Breakthrough” Eight Steps to Wellness– Life-altering Secrets from Today’s Cutting-edge Doctors”, Crown Publishers, 2008




