
Introduction
Cryptococcosis is a condition that also has the alternative diagnostic names “tolurosis” or “blastomycosis”. Notably, Cryptococcus neoformans transmits this fungal infection. It is important to realize that this pathogen exists in soil worldwide. Some patients are very sensitive to this pathogen, particularly AIDS patients, but also patients with Hodgkin’s lymphoma, patients on long term high doses of corticosteroids or sarcoidosis patients.
Another key point, the encapsulated yeast form of C. neoformans enters the body through inhalation of dust contaminated with the pathogen. In the lungs of a healthy host a self-limited cryptococcal infection would ensue. However, in AIDS patients there is a paralysis of the immune system and often a severe pneumonia develops. The infection then spreads throughout the system with skin lesions, subcutaneous nodules and disease in liver, kidneys, spleen, joints, bones, prostate and other organs. AIDS patients often come down with cryptococcal meningitis of the central nervous system.
Signs and symptoms
During the acute lung infection phase symptoms would include coughing, chest wall pain and difficulties breathing.
Skin involvement looks quite varied with pustules, papules, acne like and even with basal cell cancer-like appearance of lesions. This is shown here with two images, before and after treatment (thanks to www.scielo.br for this link, scroll down). If the physician is in doubt what the lesions are, one or two of them could be biopsied for analysis by the pathologist. Single lesions in bone, abdominal organs or kidney may not give any symptoms, because they are pain free and are self-limiting in a person with a normal immune system. Headaches, blurred vision, behavioral changes, confusion, agitation and depression can all be symptoms of a beginning cryptococcal meningitis.
Diagnostic tests
Culture from body fluid samples such as urine, blood, phlegm or cerebrospinal fluid (CSF) lead to the diagnosis. The pathologist examines smears of biopsy specimens after special staining techniques by an experienced laboratory physician or technician.
The characteristic encapsulated budding yeasts of C.neoformans with cryptococcal capsular polysaccharide have a unique appearance that can readily be distinguished from other pathogens by the experienced observer. Finally there is a latex test for capsular antigen, which is a specific blood test, particularly, if the titers are higher than 1:8. The physician examines pulmonary lesions by X-rays, CT scans, bronchoscopy with biopsy to lead to a diagnosis. With any palpable lesion such as in skin or in the subcutaneous tissue skin biopsy would be considered. With meningitis the physician does a lumbar puncture to obtain CSF in order to diagnose the condition. The biopsy material shown here shows large, pale cells, which are the Cryptococcus neoformans fungal cells invading the lung tissue.
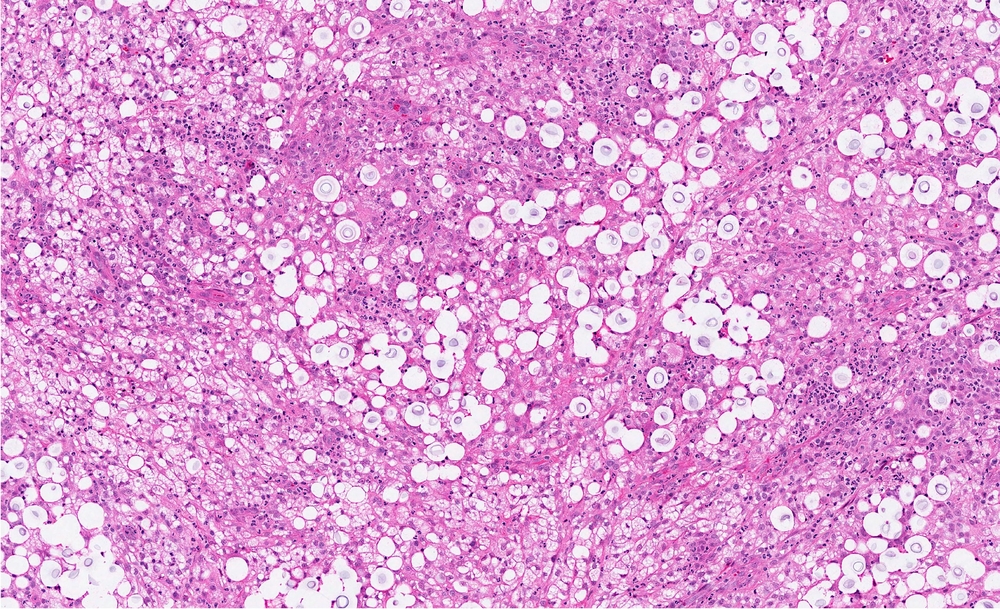
Cryptococcosis (Lung biopsy Of Patient With Cryptococcal Infection)
Treatment
The doctor individualizes treatment according to the situation. It depends whether the patient is immune-competent or immunocompromised as in an AIDS patient.
The patient with a normal immune system may not need treatment for a localized lung infection with cryptococcus, as it would often be self limiting. However, in order to be certain that the assumption of “localized disease” is correct it is wise for the physician to examine and culture the CSF (to rule out meningitis), the urine (rule out kidney involvement) and examine the skin for any abnormal lesions. Patients with a normal immune system can be treated for mild disease with fluconazole (brand name: Diflucan) orally. More severe infection would have to be treated with flucytosine (brand name: Ancobon) orally, but side-effects (kidney and bone marrow toxicity) has to be monitored. Some centers can measure flucytosine levels, which would be desirable to avoid toxic levels. Serious disease is treated with intravenous amphotericin B in combination with or followed by oral flucytosine.
References
1.The Merck Manual, 7th edition, by M. H. Beer s et al., Whitehouse Station, N.J., 1999. Chapter 158.
2.The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 113.
3. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 164.
4.David Heymann, MD, Editor: Control of Communicable Diseases Manual, 18th Edition, 2004, American Public Health Association.




