
Staging of ovarian cancer is important as it would be for any other cancer before treatment is instituted; but for ovarian cancer it is doubly important.
It is important, because nobody can predict what stage the woman with ovarian cancer is actually in until after the exploratory surgery has been completed and all the histology is in. Another complication with ovarian cancer is that there is a phenomenon called “transperitoneal dissemination.”
Even in a stage I or stage II ovarian cancer there can be leakage of cancer cells through the intact ovarian capsule, which is shed into the peritoneal fluid. Unfortunately there is an intraperitoneal flow of peritoneal fluid from the pelvic area going up through the right abdominal gutter to the right hemidiaphragm. The right hemidiaphragm, which is the border between the right upper abdominal cavity and the right chest cavity, functions like a sieve through which 80% of the peritoneal fluid gets drained into the mediastinal lymph glands and lymphatic vessels and then into the blood stream.
With these physiological facts it is now understandable how cancer from an ovarian tumor, which to the eye still appears intact (stage I or II) can shed cancer cells through transperitoneal dissemination. The cancer cells migrate through the peritoneal flow described above to the right upper abdomen, the liver, the base of the right lung and into the mediastinum. These facts are only known since the late 1980’s and following this the staging laparotomy was developed. This elaborate surgery is performed by cancer surgeons in the major Cancer Centers throughout the world. Taking into consideration the peritoneal fluid flow, there are standard points that are checked within the abdominal cavity and tissue biopsies are taken even when there is no apparent cancer. This way the microscopic spread would become apparent as the pathologist analyzes all the samples.
The surgeon will remove any ovarian cancer metastases that are obvious in a procedure called “cytoreductive surgery”, where not only the visible cancer is removed, but also the affected lymph glands are removed and sent for pathology. This removes much of the tumor load. Later on the patient is treated with the appropriate therapy (chemotherapy and/or radiotherapy).
Staging Of Ovarian Cancer
The conventional staging for ovarian cancer uses the FIGO stage grouping. There are four stages I to IV and each has three subclasses A, B and C. The higher the group or the subclass denomination, the worse the outcome(prognosis). The following brief outline explains the staging:
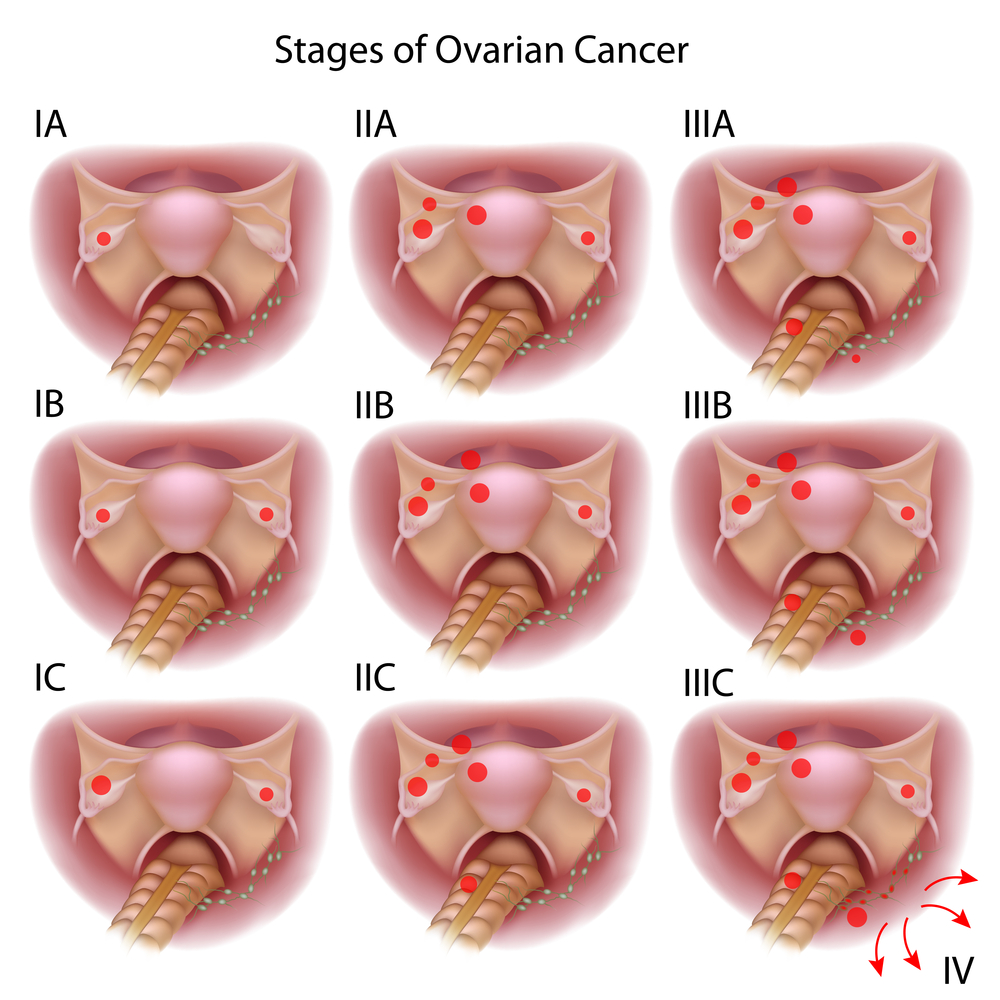
Staging of Ovarian Cancer (Figo stage)
Stage (Figo):
I A : Local tumor in one ovary
I B : Local tumor in both ovaries
I C : Tumor on surface, capsule ruptured or positive peritoneal washings
II A : Involves 1 or 2 ovaries, pelvic extension
II B : Extension to uterus and/or tubes
II C : Like IIA or IIB, but capsule ruptured, cells on surface of tubes or positive peritoneal washings
III A : Appears grossly limited to pelvic cavity, but positive for abdominal peritoneal surfaces
III B : Like IIIA, but also abdominal implants not exceeding 2cm (=3/4″) in diameter
III C : Abdominal implants greater than 2cm (=3/4″), lymph glands in groin (inguinal) or behind abdominal wall(retroperitoneal)
IV : Extensive local disease, also distant metastases in lungs, liver or pleural fluid
In addition to this staging system there is also a histological staging system (Broder classification) depending on the maturity of the cells. The higher the number, the worse the prognosis. Broder grade I has a good prognosis, but the worst would be Broder grade IV. The staging procedure takes these factors into account as well.
References:
1. V.T. DeVita et al. : Cancer- Principles & Practice of Oncology, Vol.1, 4th edition. J.B. Lippincott Co., Philadelphia, USA, 1993. Ovarian cancer chapter.
2. Cancer: Principles&Practice of Oncology. 5th edition, volume 1. Edited by Vincent T. DeVita, Jr. et al. Lippincott-Raven Publ., Philadelphia,PA, 1997. Ovarian cancer chapter.
3. S Ginath et al. Int J Oncol 2001 Jun;18(6):1133-1144.
4. Y.-L. Hu et al. J Natl Cancer Inst 2001 May 16;93(10):762-767.
5. MKTuxen et al. Br J Cancer 2001 May;84(10):1301-1307.
6. U Wagner et al. Clin Cancer Res 2001 May;7(5):1154-1162.
7. Conn’s Current Therapy 2004, 56th ed., Copyright © 2004 Elsevier
8. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc




