
Introduction
Another name for IUD is intrauterine device. Women in the US likely under-utilize these devices when compared to other countries.
Only 1 to 3% of women who use some form of contraception in the U.S. will choose IUDs and only about 80% of those who choose this method will continue at the end of the first year. It is a complex interaction that likely is responsible for this. There is a subpopulation of women who are very sensitive and who will not tolerate a foreign body in their womb.
Religious taboos
The manufacturers improved the designs and the tissue friendliness of the materials. So this point should not be a major factor any more. However, there are religious taboos for many, as many churches perceive this method of birth control as an abortion method. They claim that IUDs interfere with an early development of the pregnancy. The first cell divisions take place in the fallopian tube and the IUD prevents implantation of the early pregnancy into the lining of the uterus.
More information about IUD’s
This is exactly how the IUD works: by interfering with the implantation of the fertilized egg into the uterine cavity. By knowing the mechanism of the various contraceptive methods the couple can arrive at an informed decision and choose what is right for them. Two common IUDs are the ProgesteroneT (Progestasert IUD) and the Copper T IUD (Paragard). The newest addition to the IUDs on the market is called Mirena. This IUD device is unique and will be discussed below as it has another mechanism of action, more like an internal birth control device.
How IUDs work
The IUDs work by setting up a chronic inflammatory reaction inside the womb that is sterile, but that is toxic to sperm when they enter and attempt to swim upstream to the fallopian tube. Copper of the Copper IUD also releases local prostaglandins, which inhibit enzymes from the uterine lining amplifying the spermicidal effect. Paragard is approved for 10 years, but is likely effective for about 12 years. The Progestasert requires a change once a year as the progestin is depleted earlier.
More details regarding Mirena
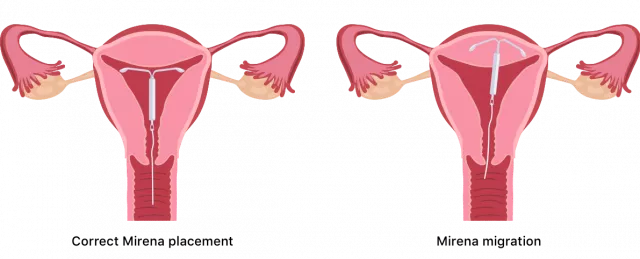
Mirena requires a change to a new one every 5 years. The manufacturer incorporated Barium sulfate into the plastic frame so that X-rays can make the IUD visible in case of migration through the uterine wall. This is a rare, but not an insignificant complication. People have exaggerated the cause of pelvic inflammatory disease, as more likely it comes from unprotected sex and symptoms of STDs rather than the IUD. IUDs only protect against pregnancy, not against VD/STD. Condoms are still recommended for prevention of sexually transmitted diseases in case of this risk. As I pointed out in another chapter on this topic, prevention of sexually transmitted disease (safe sex) is a matter of safe sex practice.
The safety record in terms of preventing pregnancy for IUDs is as good as that of tubal ligations. The advantage though is that the IUD is reversible.
Details about Mirena
This newest addition to the IUD’s consists of a small polyethylene T-shaped frame with a cylindrical reservoir around the vertical arm of the T-frame. After insertion into the womb cavity it releases a small amount of the potent progestin hormone levonorgestrel. This inhibits the development of the lining of the womb so that a pregnancy will not develop. At the same time it thickens the mucous in the cervical canal preventing passage of sperm into the womb. Trials involved more than 7600 women years in women of child-bearing age of 18 years and older. As Ref. 27 shows, at a recent conference in Vancouver/BC this IUD was felt to be the safest and most reliable IUD on the market.
Pregnancy after removal of Mirena
The other advantage is that normalcy is restored within 1 to 3 months of removing Mirena and pregnancy is easily achieved. Here is a summary of the myths that still surround IUDs and how Dr. Debra Millar (professor for obstetrics and gynecology, University of BC) explained the new research data.
The 7 Myths about IUDs and objective answers (regarding Mirena)*
- Myth: Increased risk of infection. Truth: Earlier trials were misleading; recent trials showed higher infection rates in the first 3 weeks following insertion, infection rate otherwise extremely low for years.
- Myth: Use of Copper IUDs and risk of infertility in younger women. Truth: Women who never had babies can safely use Mirena. Age and history of child birth is irrelevant. No infertility cause. STDs more common.
- Myth: Complications of expulsion and perforation through womb. Truth: Perforation at time of insertion by inexperienced physician only. Expulsion extremely rare because of cylinder size.
More myths regarding IUDs
- Myth: IUD prevents implantation of pregnancy. Truth: Newer IUDs different. Sperm not allowed in, implantation impossible.
- Myth: Cannot be used in a woman who never had a child. Truth: Women who never were pregnant included in trials. No problem of conceiving after Mirena removal.
- Myth: Excessive bleeding a problem. Truth: Mirena is used for therapy of heavy periods due to hormone influences (in other words, the opposite is true).
- Myth: Women not interested in IUDs. Truth: High %-age of patients in trials were following through. IUDs being an alternative to sterilizing procedures appealed to women as it allowed the option of a future pregnancy.
* modified from Ref. 27, lecture by Dr. Debra Millar entitled “Pearls and patches”
Chlamydia infections with several sex partners
The question of ectopic pregnancies in younger women was explained by analyzing the data of several trials. It turned out that the age group of women in the teens to age 25 have on average several sex partners in quicker succession and are at a higher risk of undiagnosed Chlamydia trachomatis infection of the cervical canal. When IUDs are inserted in this setting the infection is inadvertently spread into the womb and into the fallopian tubes. The risk of higher tubal infection and pregnancy rates is not linked to the use of IUDs (the above mentioned myth), but is due to this subgroup of women being infected with chlamydia. Conversely, young women with a steady partner who used Mirena as an IUD had no problems tolerating the system, had no infections and had also no problem becoming pregnant normally only a few month after removal of the IUD.
Summary
Mirena is a safe, effective and estrogen free, reversible birth control method. It needs to be inserted by a gynecologist or a well-trained general practitioner who does a lot of IUD insertions. In a first visit a pelvic examination is done with a Pap test and a cervical swab to rule out infections.
In a second visit the IUD is inserted after premedication with misoprostol, a vaginal suppository that softens the cervix and makes the insertion of the IUD easier. When it is placed, there will be one more follow-up visit to ensure that the IUD has stayed in place. However, following this there is nothing to worry about for 5 years at which time the IUD has to be replaced with a new one.
No risk of stroke or heart attack with IUDs
There are no risks of strokes or heart attacks unlike with oral contraceptives. All of the effects are local with no systemic effects. Even women who had prior complications such as previous C-sections, ectopic pregnancies, pelvic inflammatory disease history, or blood clots in veins can safely take Mirena (Ref. 27). The woman with an IUD in place still needs regular Pap smear tests for cervical cancer screening and needs to protect herself with barrier methods against possible exposure to sexually transmitted diseases.
References
1. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 235.
2. B. Sears: “Zone perfect meals in minutes”. Regan Books, Harper Collins, 1997.
3. Ryan: Kistner’s Gynecology & Women’s Health, 7th ed.,1999 Mosby, Inc.
4. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 245.
5. AB Diekman et al. Am J Reprod Immunol 2000 Mar; 43(3): 134-143.
6. V Damianova et al. Akush Ginekol (Sofia) 1999; 38(2): 31-33.
7. Townsend: Sabiston Textbook of Surgery,16th ed.,2001, W. B. Saunders Company
8. Cotran: Robbins Pathologic Basis of Disease, 6th ed., 1999 W. B. Saunders Company
More references
9. Rakel: Conn’s Current Therapy 2001, 53rd ed., W. B. Saunders Co.
10. Ruddy: Kelley’s Textbook of Rheumatology, 6th ed.,2001 W. B. Saunders Company
11. EC Janowsky et al. N Engl J Med Mar-2000; 342(11): 781-790.
12. Wilson: Williams Textbook of Endocrinology, 9th ed.,1998 W. B. Saunders Company
13. KS Pena et al. Am Fam Physician 2001; 63(9): 1763-1770.
14. LM Apantaku Am Fam Physician Aug 2000; 62(3): 596-602.
15. Noble: Textbook of Primary Care Medicine, 3rd ed., 2001 Mosby, Inc.
16. Goroll: Primary Care Medicine, 4th ed.,2000 Lippincott Williams & Wilkins
Further references
17. St. Paul’s Hosp. Contin. Educ. Conf. Nov. 2001,Vancouver/BC
18. Gabbe: Obstetrics – Normal and Problem Pregnancies, 3rd ed., 1996 Churchill Livingstone, Inc.
19. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 251.
20. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 250.
21. Ignaz P Semmelweiss: “Die Aetiologie, der Begriff und die Prophylaxis des Kindbettfiebers” (“Etiology, the Understanding and Prophylaxis of Childbed Fever”). Vienna (Austria), 1861.
Final references
22. Rosen: Emergency Medicine: Concepts and Clinical Practice, 4th ed., 1998 Mosby-Year Book, Inc.
23. Mandell: Principles and Practice of Infectious Diseases, 5th ed., 2000 Churchill Livingstone, Inc.
24. Horner NK et al. J Am Diet Assoc Nov-2000; 100(11): 1368-1380.
25. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
26. Rakel: Conn’s Current Therapy 2004, 56th ed., Copyright © 2004 Elsevier
27. The 50th Annual St. Paul’s Hospital Continuing Medical Education Conference for Primary Physicians, Nov. 16 – 19, 2004





{kind=link}