
Introduction
Kidney stones (medically termed “renal calculi”)can slowly develop unnoticed in the center part of the kidney called renal pelvis. However, when the stone breaks loose and migrates through the ureter from the kidney to the bladder, the patient suddenly becomes very sick with excruciating pains (renal colic). About 1 of every thousand patients ends up with an admission to hospital.
Of all autopsies for other disease, the pathologist will find a kidney stone in 1% of the autopsies. About 20% of patients with gout develop kidney stones.
Kidney stone symptoms
Usually there is back pain initially, which irradiates into the right upper abdomen. This is the type of pain the patient experiences when the stone is fairly high at the beginning of the ureter.
As the stone travels down, the sharp edges can injure the ureter and blood appears in the urine (called “hematuria”). The quality of the pain becomes stronger and very rhythmic like labor pains. This is because the ureter is made up of the same smooth muscle tissue as the uterus and physiologically, when a foreign body (baby or stone) is expelled against resistance the smooth muscle will have rhythmic contractions. Eventually when the stone arrives close to the bladder, the pain is in the lower right or left abdomen (depending on which side the stone is) and radiates into the genital region and the inner thigh area on the affected side.
Abdominal pain may mask real diagnosis of kidney stone
As a large part of the ureter on the back wall of the abdomen is coated with the same peritoneal membrane that coats all internal abdominal organs, similar gastrointestinal symptoms can mask the real diagnosis. This explains why a patient can suddenly vomit from the peritoneal irritation, get extension and bloatedness of the abdomen with signs very similar to those of bowel obstruction.
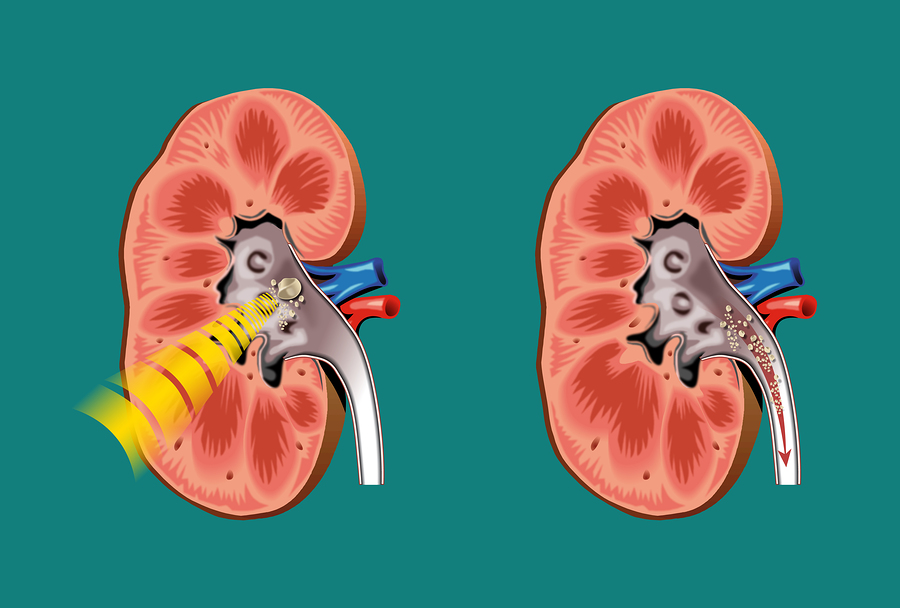
Kidney Stones (Treated with Lithotripsy On Left)
Kidney stone treatment
Usually a patient with these excruciating symptoms will present at the Emergency Room of a hospital. Pain relief is in the foreground as this will also facilitate the passing of the stone. Most small stones will pass within a few hours, others might do so within two or three days.
When urine is put through a strainer, the passed stones can be recovered and analyzed. About 80% contain calcium (mostly as calcium oxalate), about 5% are uric acid stones, the remainder are of a variety of salts. Magnesium ammonium phosphate stones are associated with chronic urinary infections where the bacteria split urea and form this type of stone, which is very common in women. Plain X rays and non contrast spiral CT scan will diagnose most kidney stones, the rest can be visualized by other diagnostic techniques (intravenous urography).
Shock wave lithotripsy
If the stone does not pass within three days, the urologist has several options of extracting it. Shock wave lithotripsy is the method of choice for most stones less than 2 cm (=0.8″) in diameter. With this treatment energy from the lithotripsy machine focuses on the stone until it shatters into smaller pieces. The urologist repeats the procedure until the stone has disintegrated into sand like particles, which easily pass. The specialist removes any remaining smaller stones via endoscopic techniques. When the approach is through the skin the name of the procedure is “percutaneous nephrolithotomy” or kidney stone operation. When the approach is through the bladder and the ureter the name of the procedure is “ureteroscopy”. Other surgical techniques exist as well as does a chemical dissolving method. To establish, which method is best to use is up to the urologist.
Special diet for kidney stone prevention
The doctor may have special diet suggestions as to what to avoid and what to add in the diet to prevent recurrence of a kidney stone. This will depend on the stone analysis.
References
1. DM Thompson: The 46th Annual St. Paul’s Hospital CME Conference for Primary Physicians, Nov. 14-17, 2000, Vancouver/B.C./Canada
2. C Ritenbaugh Curr Oncol Rep 2000 May 2(3): 225-233.
3. PA Totten et al. J Infect Dis 2001 Jan 183(2): 269-276.
4. M Ohkawa et al. Br J Urol 1993 Dec 72(6):918-921.
5. Textbook of Primary Care Medicine, 3rd ed., Copyright © 2001 Mosby, Inc., pages 976-983: “Chapter 107 – Acute Abdomen and Common Surgical Abdominal Problems”.
6. Marx: Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th ed., Copyright © 2002 Mosby, Inc. , p. 185:”Abdominal pain”.
7. Feldman: Sleisenger & Fordtran’s Gastrointestinal and Liver Disease, 7th ed., Copyright © 2002 Elsevier, p. 71: “Chapter 4 – Abdominal Pain, Including the Acute Abdomen”.
8. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
9. Suzanne Somers: “Breakthrough” Eight Steps to Wellness– Life-altering Secrets from Today’s Cutting-edge Doctors”, Crown Publishers, 2008




