
Introduction
Normally there is no pathogen in urine, in other words urine is sterile. In children there is usually a structural congenital abnormality, if there is an infection. Women in their middle age outnumber men by a factor of 50-fold in frequency of bladder infections. In the age group of older than 50 years, when prostate hypertrophy becomes an important factor in males, more males get bladder infections.
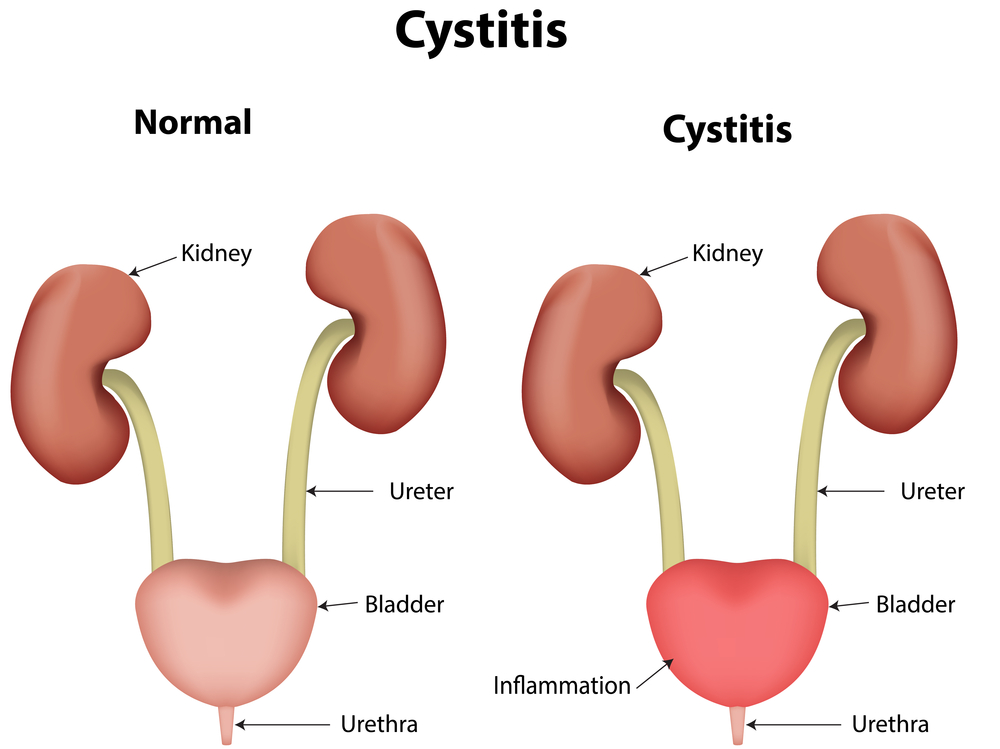
Although we talk about “bladder infection”, the truth is that the infecting agents are opportunists and do not know where the limit of the bladder is. Although there might be a start in the bladder, the bacteria very quickly ascend via the ureter and lymphatic connections and cause a kidney infection. This leads to pyelonephritis (see “pyelonephritis” under “abdominal pain”).
We call the infection of the urinary tract system simply URI (=urinary tract infection) and this includes cystitis (bladder infection), urethritis (infection of the urethra) and pyelonephritis.
Here is a breakdown of the common bugs found in patients with UTI’s found in either the office setting or the hospital setting:
Comparison of bacteria found in urine samples of patients with UTI’s in the office or hospital setting
| Type of bacterium: | Office setting: | Hospital setting: |
| Escherichia coli( the main bacterium of the colon and rectum) | 80% | 50% |
| Staphylococcus saprophyticus | 10% | 2% |
| Klebsiella, Enterobacter, Proteus and Serratia | 0% | 40% |
| Enterococcus faecalis, Staph. saprophyticus and aureus | 0% | 5% |
| Other bacteria | 10% | 3% |
It is clear from this table that the patient population in the hospital is quite different from the population seen in the typical office setting. Klebsiella and related species are typically found in patients who are having chronic problems with their kidneys, ureters and bladders. They are older people and people who suffer from other illnesses and recurrent kidney stones.
Urinary Tract Infection Symptoms
While an infection of the urethra is mild and comes on gradually, the onset of a bladder infection is abrupt with frequent and painful urination. There is a stinging, burning feeling when urinating, but the amounts of urine each time are very small. Even when the bladder is empty, it feels as if there would be more urine in the bladder. About 1/3 of patients with a cystitis have blood in the urine, which originates from the inflamed bladder wall. There is a burning pain just above the pelvic bone deep inside the lower mid abdomen.
Bladder Infection
Urinary Tract Infection Treatment
The doctor will likely order a mid stream urine sample to be sent to the lab for a culture and sensitivity test. This tells the doctor what bacteria grew and to which antibiotic they are sensitive or resistant to. In the meantime, when the sample has been taken, an antibiotic is prescribed.
As about 30% to 50% of patients with bladder infections also have silent kidney infection (pyelonephritis), the doctor will likely choose an antibiotic, which at the same time would eradicate a kidney infection. Two common antibiotics used as an initial therapy while awaiting cultures are trimethoprim-sulfamethoxazole (brand names: Bactrim, Sulfatrim, Septra) or ciprofloxacin (Ciloxan, Cipro). Often the culture and sensitivity report will confirm that the antibiotic chosen was correct. But if the patient did not get better in a few days and the results suggest that another antibiotic would likely have a better response, the doctor can prescribe the antibiotic that fits based on the sensitivity test. Occasionally a urethritis or bladder infection can be part of venereal disease and another antibiotic has to be prescribed for that.

Bladder Infection (Petri Dish With Urinary Culture)
Follow-up exams may be necessary to ensure that there is no venereal disease elsewhere in the body. The doctor needs to remember that recurrent UTI’s have an underlying reason and may need a referral to a urologist. One common congenital reason for UTI’s in children of the 1 to 5 year-old group is a vesico-ureteral reflux (=urine flows backwards from the bladder into the urethra) because of a weak valve in that area. X-ray studies need to be organized and the urologist needs to do a reimplantation surgery of the ureter. This surgery has helped many children to never develop chronic pyelonephritis, which used to be and still is a main reason for the need of dialysis or the need for kidney transplants in the end stage.
References:
1. DM Thompson: The 46th Annual St. Paul’s Hospital CME Conference for Primary Physicians, Nov. 14-17, 2000, Vancouver/B.C./Canada
2. C Ritenbaugh Curr Oncol Rep 2000 May 2(3): 225-233.
3. PA Totten et al. J Infect Dis 2001 Jan 183(2): 269-276.
4. M Ohkawa et al. Br J Urol 1993 Dec 72(6):918-921.
5. Textbook of Primary Care Medicine, 3rd ed., Copyright © 2001 Mosby, Inc., pages 976-983: “Chapter 107 – Acute Abdomen and Common Surgical Abdominal Problems”.
6. Marx: Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th ed., Copyright © 2002 Mosby, Inc. , p. 185:”Abdominal pain”.
7. Feldman: Sleisenger & Fordtran’s Gastrointestinal and Liver Disease, 7th ed., Copyright © 2002 Elsevier, p. 71: “Chapter 4 – Abdominal Pain, Including the Acute Abdomen”.
8. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.




