
In the first place, with primary osteoporosis cases diagnostic tests for osteoporosis chiefly consist of simple blood tests. First calcium, second phosphate, third alkaline phosphatase levels, further red blood cell sedimentation rate and finally serum electrophoresis will be ordered by the physician. Ultimately most of these tests often are normal.
With this in mind, type I osteoporosis indeed has an association with high FSH, low estrogen and low progesterone in women and surely with low testosterone in males. To clarify, both males and females, of course have a hormone deficiency pattern of hypogonadism with this type of osteoporosis (see Ref. 8).
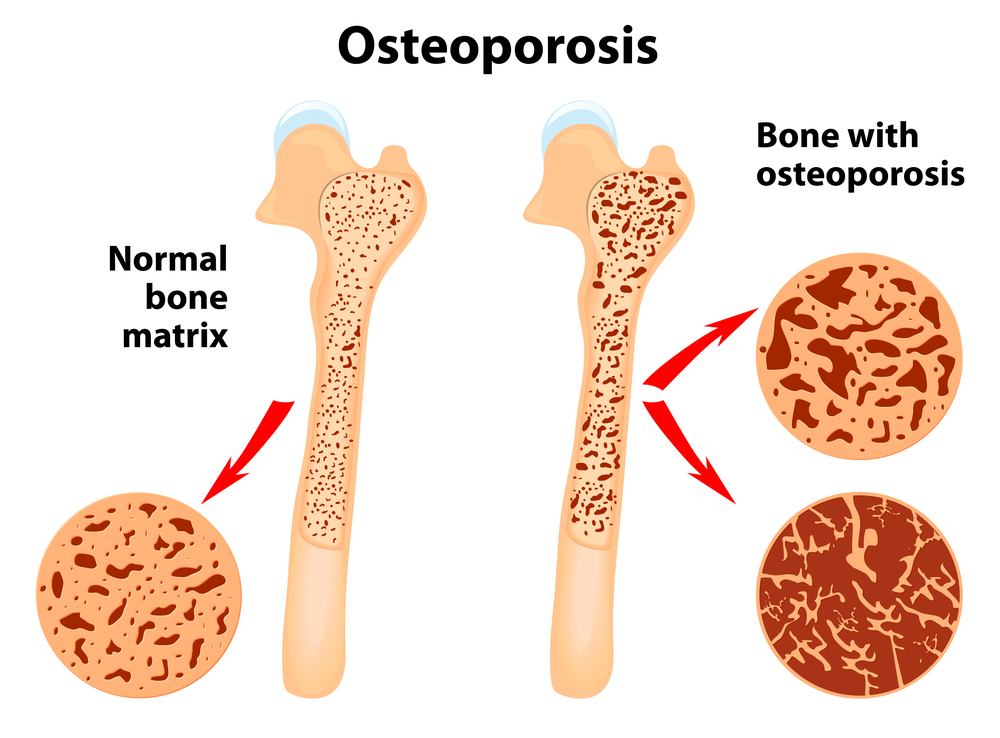
In like manner, type II osteoporosis usually has an association with vitamin D3 deficiency. Most noteworthy, we know from research papers that there is indeed a lowered number of bone building cells in the bone. This leads to a disbalance such as bone production and bone turnover with an overall net bone loss. Notably, the ultimate test for determining the amount of bone mass loss is particularly with the help of dual-emission X-ray absorptiometry (for short: DEXA or DXA).
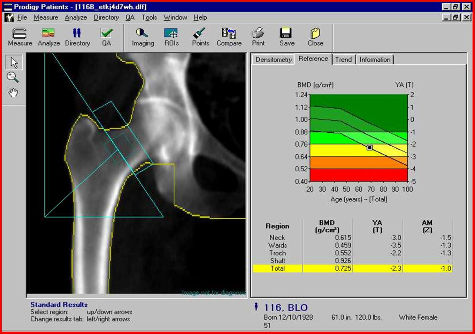
DEXA scan
Certainly, the DEXA scan is done easily at any X-ray department (Ref.1). Above all, the physician expresses the results according to the outline in the beginning of the chapter on osteoporosis, as standard deviations below the norm of 35-year old control persons. These are matched for sex and race.
Moreover, it is important to realize that when Fosamax came out for osteoporosis treatment by Merck in 1995 there were two probably independent occurrences that helped the marketing of Fosamax (see Ref. 9). First, the WHO came out with a then new definition of osteoporosis where the bone density of a 30-year old woman was the new reference point. By all means, this new criterion immediately declared 30% of postmenopausal women to have osteoporosis. Second, Merck subsidized of course the distribution of machines to test bone density. Above all, this bone density test provided the physician with a powerful tool to assess the risk for a fracture in the near future. In the light of marketing Fosamax, this motivated Merck to get involved in sponsoring DEXA machines.
Lower and higher bone density
On the one hand this relationship would be similar to measuring blood pressure and predicting how likely it would be for the patient to get a stroke. It has been determined in a group of patients with osteoporosis that the difference in probability between the lower density and higher density patients on the DEXA test to develop a hip fracture was 8.5-fold higher (Ref.1) in the low bone density group. However, there are some problems with Fosamax as will be discussed under “treatment of osteoporosis”.
Secondary osteoporosis
Generally speaking, in secondary osteoporosis the doctor orders blood tests that uniquely help to distinguish between the specific hormone imbalances and other causes. For instance, a positive history of celiac disease would likely result in a referral of the patient to the gastroenterologist for a further work-up. On the contrary, the doctor may refer the patient to a rheumatologist in the case of a patient with an underlying rheumatological disease. In that case the patient may have rheumatoid arthritis or ankylosing spondylitis.
Likewise, a suspicion for cancer would trigger the physician to order a nuclear medicine bone scan and other imaging techniques coupled with additional blood tests. Finally, a history of drug use should be taken as this can interfere with the patient’s bone metabolism. For one thing, prednisone taken for asthma or a rheumatic disease can have the side effect of osteoporosis. Overall, for example, alcohol and smoking are also powerful negative factors as was mentioned above.
Diagnostic Tests For Osteoporosis
Here is a summary in tabular form of the tests that are done (Ref. 1 and 2) to investigate for osteoporosis.
Diagnostic tests for osteoporosis
_____________________________________________________________
X-rays : requires 30% bone loss to show as osteopenia; good for compression fractures of vertebral bones or fractures of trabecular bone
DEXA (dual-emission X-ray absorptiometry) : the gold standard to measure bone density
serum calcium : rule out hyperparathyroidism (if elevated measure parathyroid hormone)
serum protein electrophoresis : rule out multiple myeloma (if positive, check urine for Bence-Jones protein)
T4, TSH : rule out hyper- or hypothyroidism
serum cortisol : rule out Cushing syndrome
serum testosterone : rule out malfunctioning of testicles
FSH, LH : in women, rule out premature menopause
indicators of bone turnover (not routinely used) : special tests like technetium-99m methylene diphosphonate etc. can be utilized
bone marrow biopsy : distinguishes between osteomalacia (vitamin D deficiency) and osteoporosis, but is an invasive test
_____________________________________________________________
References
1. ABC of rheumatology, second edition, edited by Michael L. Snaith M.D., BMJ Books, 1999.
2. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 57.
3. B. Sears: “The age-free zone”.Regan Books, Harper Collins, 2000.
4. B. Sears: “Zone perfect meals in minutes”. Regan Books, Harper Collins, 1997.
5. Goldman: Cecil Textbook of Medicine, 21st ed.(©2000)W.B.Saunders
6. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
7. Rakel: Conn’s Current Therapy 2004, 56th ed., Copyright © 2004 Elsevier
8. Dr. John R. Lee: Natural Progesterone- The remarkable roles of a remarkable hormone”, Jon Carpenter Publishing, 2nd edition, 1999, Bristol, England.
9. Michael T. Murray, N.D.: “What the drug companies won’t tell you and your doctor doesn’t know” – The alternative treatments that may change your life – and the prescriptions that could harm you. Atria Books (subsidiary of Simon & Schuster Inc.), 2009.





{kind=link}