
Introduction
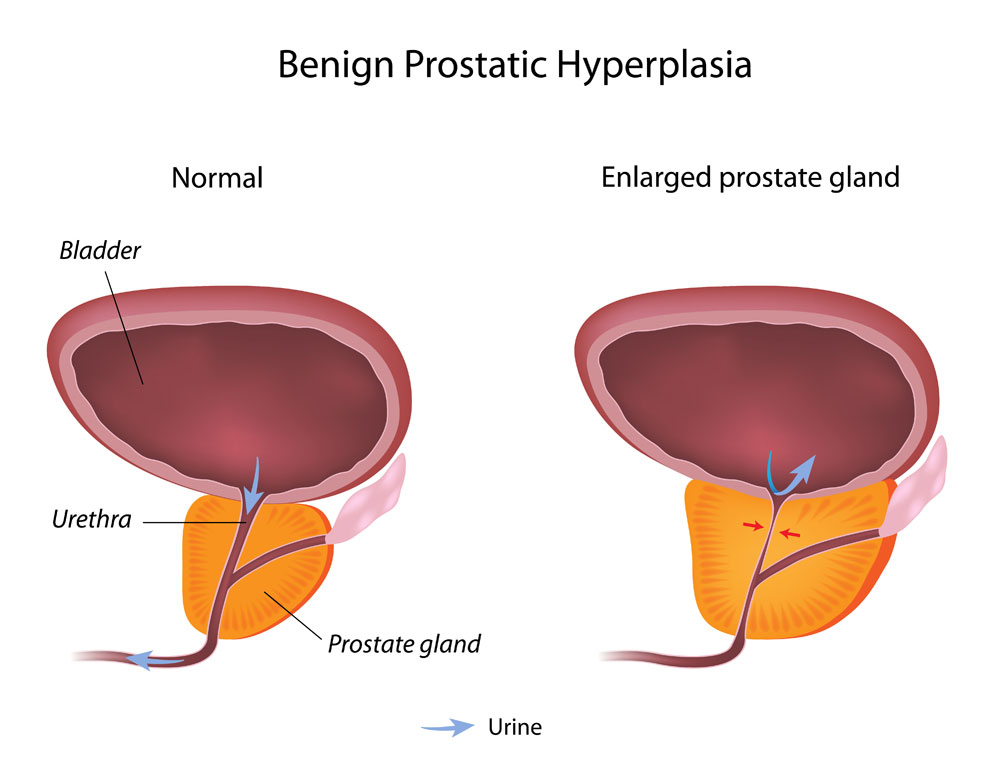
Prostatic hypertrophy means that there is an enlargement of the prostate gland. Other names for this condition are benign prostatic hypertrophy or BPH; another name is “benign prostatic hyperplasia”. We know from autopsy studies that an prostate enlargement is a common occurrence in males, particularly as they age. Bladder outlet obstruction from a benign enlargement of the prostate slows down the urinary flow. This is age-related as I am discussing below.
Prostate enlargement as a function of age
| Age group: | Percentage of men with an enlarged prostate: |
| 31 – 40 | 10% |
| 41 – 50 | 45% |
| 51 – 60 | › 80% |
Not every man with prostate enlargement requires treatment, only those men who develop symptoms of urinary obstruction. Once the urine flow slows down to less than 600 ml per minute, critical situations can develop. For instance, after a few beer urinary volume increases significantly. Medications that have subtle anticholinergic side-effects lead to more urinary flow obstruction.
Prostatic Hypertrophy
The involuntary bladder function ensures that the bladder wall automatically relaxes. If the bladder is full , it transmits signals that indicate to you an urge to go to the bathroom. The powerful parasympathetic nerve is what controls the bladder function. The biochemical transmitter in this part of the autonomic nervous system is acetylcholine. That’s why physicians call the transmission mode “cholinergic” and anything that inhibits it “anticholinergic”. There are a great number of very diverse medications that have anticholinergic side-effects. Many of them are available over the counter. All of them inhibit the parasympathetic nerve function.
There is nothing wrong about these medications. However, it is important to know that even minor anticholinergic side-effects of various medications that the patient may take, can add up. This effect is amplified in the elderly and in particular in elderly men. It is in elderly men that a high percentage have a partial blockage of the urethra from prostate enlargement. As the urethra squeezes itself through a prostate enlargement, there can be suddenly a complete closure of the urethra. This causes hospitalization of a patient like this. The diagnosis is usually an acute urinary retention. Here is an example of such a patient.
A patient with benign prostatic hypertrophy (=BPH)
____________________________________________________________________
Mr. Smith is a 55 years old salesman for a car company. Physicians diagnosed him in the past with GERD (gastro-esophageal reflux disease). For this he takes ranitidine 150 mg twice a day. He also belongs into the age group who often have a benign prostatic hypertrophy (BPH). The doctor diagnosed this with a screening test for prostate cancer (PSA), which had been in the 20 IU range.
His doctor sent him to a urologist, who did a series of prostate biopsies, which did not show cancer. However, the tests confirmed BPH. This patient also went through a stressful part in his life and was put on an antidepressant called trazodone. The patient subsequently had a cold. He decided to get some over-the-counter antihistamine (Chlor-Tripolon) and that’s when things suddenly happened.
Bladder retention caused abdominal pains
He had already felt some pressure in his lower mid abdomen for a few weeks. Now after a few beers he suddenly could not pass any urine, but had a strong urge to go. His lower abdominal pain got really severe. He also felt flank pain on each of his sides. The patient was seen at a hospital and the physician admitted him. The physician placed a suprapubic bladder catheter. He also stopped some of the medications (Chlor-Tripolon, and the trazodone) and soon he was able to void again. However, more tests were done and the urologist decided that a TURP was required. TURP stands for “transurethral resection of the prostate”. Within a few days he could leave the hospital. Now he knew that he would no longer get into problems with his BPH.
____________________________________________________________________
Here is the explanation regarding this patient
This is an example where several negative factors mounted on top of each other. Because of the age related BPH his urinary flow rate was reduced below the 600 ml/minute threshold.
He also had a variety of conditions that he could not necessarily control. Ranitidine, trazodone and antihistamines all have anticholinergic side-effects. This is super additive and leads to an intolerance of the diuretic push from by a few beers. In this patient there was a situation where the physicians decided to improve the urethral flow with a TURP. The reason was that the physician could not keep the patient completely off all of the medications. Presently he still takes ranitidine and trazodone, but has no problems with the urine flow. His kidneys are protected from hydronephrosis and eventual pyelonephritis and renal failure. Unfortunately, many patients wait until it is too late and the kidney damage is irreversible.
Symptoms
Symptoms of an enlarged prostate are more frequent urination, which over time is getting worse. With every urination the urine amounts become smaller on each trip to the bathroom. This leaves the patient with a feeling of urgency all the time. The patient also has to get up several times during the night (=nocturia).
The urinary stream is smaller in diameter and has less force. When the patient measures the volume per minute, it clearly deteriorates over time. This is directly due to the clamping down of the rubbery prostate gland enlargement around the upper portion of the urethra.
Physical findings with BPH
This leads to retention of urine in the bladder, which can balloon considerably and this is felt as suprapubic pain (central lower abdominal pain). As the patient is more prone to urinary tract infections, this too can be a signal for the physician to check this patient for BPH.
On rectal examination the physician finds a rubbery prostate gland enlargement. However, it is not hard as would be the case in prostate cancer. Blood test are done to look for kidney function and a PSA level. In 30% to 50% of BPH there is PSA elevation, which makes it difficult to delineate from prostate cancer where the PSA is positive in 30% to 95%, depending on the tumor size. The urologist usually does some prostate biopsies to differentiate between these two conditions.
BPH Treatment
The physician treats milder cases of BPH with medication such as finasteride (brand name: Proscar), terazosin (brand name: Hytrin), doxazosin (brand name: Cardura) or tamsulosin (brand name: Flomax). Unfortunately all these medications require the patient to take them life long, which makes this approach less attractive.
Surgical approaches for BPH
Surgery is the other approach. However, many men are afraid of losing their potency (=ability to have a penile erection). With the conventional TURP method (transurethral resection of the prostate) the rate of impotence is about 5% to 10%. However, with the laser beam methods there is only a rate of impotence of about 3 to 4 %. With the radio frequency thermal therapy of the prostate by transurethral needle ablation (=”TUNA”) the impotence complication rate is less than 2%. Here essentially heat is used to destroy the prostatic tissue immediately adjacent to the urethra without damage to the urethra. The patient who is affected with BPH should discuss all these options with the treating urologist. The gold standard is still the original TURP, but technological advances led to significant improvements since then.
Hormones and BPH
As men age, there is a gradual loss of testosterone and progesterone production from the testicles and the adrenal glands. On the other hand as the man ages, there are more sex hormone binding globulins, which keep these hormones bound and reduces the free hormone portion even more. In addition many men have a sagging, bulgy stomach (from overeating, too much beer and lack of exercise). Excess fatty tissue contains an enzyme, called “aromatase”, which produces estrogens out of circulating male hormones. The end result is a lack of male hormones, too much circulating estrogen and a lack of progesterone. Progesterone is what keeps excess estrogen at bay. Dr. John Lee calls this hormone constellation “estrogen dominance” (Ref. 10). He explains that this is the real reason for the enlargement of the prostate in the aging man.
High estrogen levels cause BPH and prostate cancer
Dr. Lee further explains that over the long run this can lead to the development of prostate cancer. For decades physicians believed that a surplus of testosterone would be responsible for the development of prostate hypertrophy and prostate cancer. In the mid 1940’s Dr. Charles Huggins observed that castration reduced testosterone levels. At that time, it was not known that castration also removes a man’s estrogen production, as nobody thought about testing a man’s blood for female hormones. When saliva hormone tests and blood insulin tests are done, it is clear that with the metabolic syndrome (=insulin resistance) often testosterone and progesterone levels are low, but estrogen levels are high. These men are at a high risk of developing BPH and prostate cancer.
Hormone treatment with bio-identical hormones
It follows from this that a restoration of these dysbalanced hormones to a new hormone balance improves the outlook of an aging man. The physician replaces what is missing (testosterone and progesterone). High insulin levels are reduced by Metformin and exercise/food changes (cut out sugar, starch and reduce fat intake). Doing these things can often avoid a TURP for BPH. In addition, the aging man can also avoid the development of prostate cancer. At the same time the desire for sex and normal sexual performance return as in a younger man (through the magic of hormone balance).
I like to add that not every physician feels comfortable with this approach that comes from the new branch of anti-aging medicine. You may have to search for an anti-aging physician to get a prescription for the appropriate bio-identical hormone creams.
References
- DM Thompson: The 46th Annual St. Paul’s Hospital CME Conference for Primary Physicians, Nov. 14-17, 2000, Vancouver/B.C./Canada
- C Ritenbaugh Curr Oncol Rep 2000 May 2(3): 225-233.
- PA Totten et al. J Infect Dis 2001 Jan 183(2): 269-276.
- M Ohkawa et al. Br J Urol 1993 Dec 72(6):918-921.
- Textbook of Primary Care Medicine, 3rd ed., Copyright © 2001 Mosby, Inc., pages 976-983: “Chapter 107 – Acute Abdomen and Common Surgical Abdominal Problems”.
More references
- Marx: Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th ed., Copyright © 2002 Mosby, Inc. , p. 185:”Abdominal pain”.
- Feldman: Sleisenger & Fordtran’s Gastrointestinal and Liver Disease, 7th ed., Copyright © 2002 Elsevier, p. 71: “Chapter 4 – Abdominal Pain, Including the Acute Abdomen”.
- Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
- Suzanne Somers: “Breakthrough” Eight Steps to Wellness– Life-altering Secrets from Today’s Cutting-edge Doctors”, Crown Publishers, 2008
- John R. Lee: “Hormone Balance for Men – What your Doctor May Not Tell You About Prostate Health and Natural Hormone Supplementation”, © 2003 by Hormones Etc.




