
Infectious mononucleosis, infectious mono or “kissing disease”, how it has sometimes been called, is a form of severe tonsillitis, but also is a protracted systemic viral illness and can have some hidden implications in the development of nasopharyngeal cancer in the Chinese population who have a genetic weakness for this type of rare cancer.
Epstein-Barr virus (EBV), the cause of infectious mononucleosis, is also a triggering agent for the 20 to 30 fold higher incidence of nasopharyngeal cancer in the Chinese when compared to the low rates of North Americans and Europeans (Ref. 4, p. 1774).
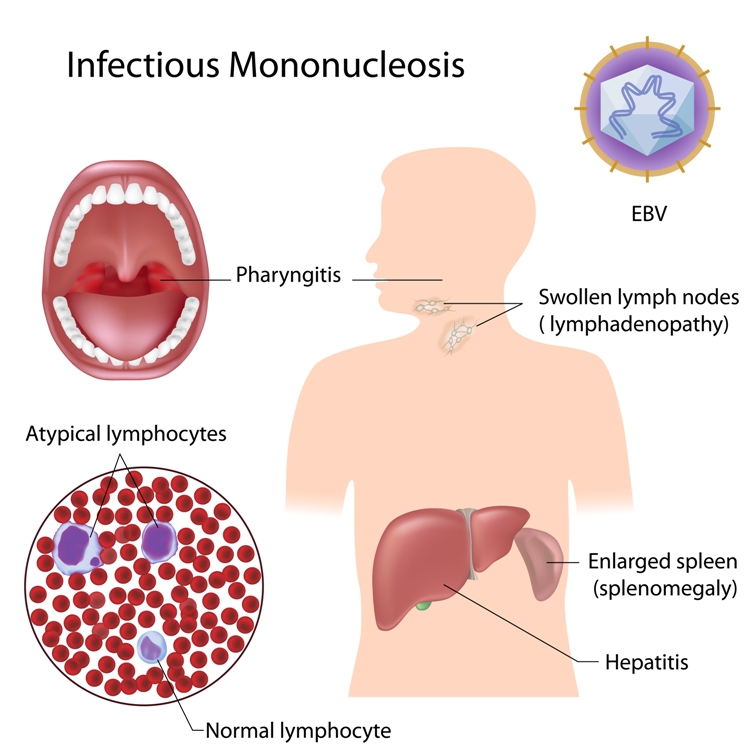
Signs and symptoms
The symptoms of EBV infection are as varied as the age group that gets affected by it. The most severe infections occur in the age group of 15 to 25. Originally researchers described the occurrence of mononucleosis among a group of college students. This was where the terminology of “kissing disease” came from. Kissing can be a source of transmission, although most of the time simple droplet infection like in any other respiratory infection is the common mode of transmission. In children the symptoms can be very mild like a cold of 1 or 2 weeks.
Young adults often have a more severe course with mononucleosis
In young adults, however, it can be a severe infection with a high fever, severe throat pain with lymph node swelling in the neck region, a viral tonsillitis and pharyngitis. The infected person may also suffer from a complete loss of appetite, nausea, abdominal pain, headaches, chills and muscle pains. In 30 % of patients there is swelling around the eyes (“periorbital edema”).
When antibodies appear in the blood in the second week there can be sometimes a skin rash that can look quite varied. Sometimes it looks like the measles, particularly when the physician started the person on amoxicillin. At other times it looks like a rash with a multitude of pin sized red spots (petechial rash).
Monitor spleen to avoid splenic rupture
The spleen is enlarged in 50% of cases, the liver only in 10%. At the end of the first week or in the second week there is a risk that the enlarged spleen could rupture with sudden jarring motions. This is why contact sports should be avoided for at least 3 weeks. The player would not perform well anyways because the EBV infection is taking a lot of energy away from the person. Viral shedding from the pharynx goes on for up to 18 months following infection with EBV! This is the case, even when the person feels recovered after 3 or 4 weeks. The reason why EBV is so common, is the fact that there are many asymptomatic carriers in the population all the time, who shed the virus by droplet transmission.
Infectious Mononucleosis
Diagnostic tests
The physician makes the diagnosis mainly on clinical grounds, by history and examination.
The blood tests confirm some typical changes such as a moderately elevated white blood cell count with 50% lymphocytes and 10% or more “atypical lymphocytes” (=the “mononucleosis cells”). By the end of the 3rd week the monospot blood test is positive in about 90% of patients (Ref. 4, p.268). This is not too specific as chickenpox, lymphomas and influenza can lead to a falsely positive monospot test as well. In these cases a EBV antibody level can be ordered, which is specific for EBV infection. After 3 months the monospot test returns to normal whereas the EBV antibody test stays positive for the rest of the life of the individual.
Treatment
Most patients recover spontaneously from EBV infection in a course of 3 to 4 weeks. There is no vaccination for it. In 1% or less of cases there can be neurological complications like seizures or aseptic meningitis.
In a May 2014 review a simple high dose intravenous vitamin C infusion was found to be effective in reducing inflammatory antibodies of EBV with associated improvement of symptoms in 91% of treated patients.
Hemolytic anemia, kidney failure, myocarditis or splenic rupture in the 2nd or 3rd week of the disease are other rare complications.
The physician rules out other underlying conditions
With large tonsils where there is a danger of airway obstruction and in cases where the platelet count is too low, the physician gives a course of corticosteroids for 1 or 2 weeks (Ref. 4, p. 268). It is wise to do a throat swab, if there is a change in the clinical presentation (more of a sore throat, worsening of the condition) to rule out a bacterial superinfection with group A beta-hemolytic streptococcus, which would need to be treated with antibiotics.
In 2006 an interesting case study reported marked improvement of symptoms with the anti-herpes drug acyclovir (Valtrex): http://www.askdrray.com/herpes-medication-successful-in-mononucleosis/
References
1. James Chin et al., Editors: Control of Communicable Diseases Manual, 17th edition, 2000, American Public Health Association.
2. Behrman: Nelson Textbook of Pediatrics, 16th ed., 2000, W. B. Saunders Company
4. Noble: Textbook of Primary Care Medicine, 3rd ed.,2001 Mosby, Inc.
5. Abeloff: Clinical Oncology, 2nd ed.,2000,Churchill Livingstone, Inc.
6. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
7. Rakel: Conn’s Current Therapy 2004, 56th ed., Copyright © 2004 Elsevier




