
Introduction
Cholelithiasis, which is also commonly termed “gall stones” usually develops over a long period of time. About 20% of U.S. Citizens over the age of 65 have gall stones and every year more than 500,000 have a gall bladder surgery (cholecystectomy).
The following are risk factors to get gall stones: first of all obesity, furthermore being of female sex, in addition older age, another risk are genetic factors (North American Indian descent, positive family history of mother or father having had a cholecystectomy) and finally, being on a Western diet.
Keeping cholesterol in solution
There is a delicate balance between the bile salts that attempt to keep the cholesterol in bile in solution and the cholesterol wanting to precipitate out when it is being concentrated inside the gallbladder. The Western diet contains something, which interferes with this delicate balance, but not everybody is sensitive to these factors. We do not know the details of these mechanisms. However, we know from long term studies that there are initially very small seed like crystals of cholesterol, which in time grown by forming layers of more cholesterol around it until there are only a few larger stones left after years and years of growth.
Mechanism of developing gallstones
This process can span over 15 or 20 years, possibly without any symptoms. Thomas et al. in London/England (Ref.3) have published evidence that constipation leads to overgrowth of anaerobe bacteria, which produce a type of bile acid that finds its way into the bile of these patients and furthers this process of precipitation of cholesterol. Further research found that deoxycholic acid (the name of this bile acid) is the common denominator in patients with cholesterol gallstones. All of the samples of bile from such patients showed a high content of this bile acid and in the stool samples showed a high growth of these anaerobic bacteria producing this bile acid as well. This confirms what many researchers have postulated for years, that constipated and obese patients were at a higher risk to develop gallstones.
Gall stone symptoms
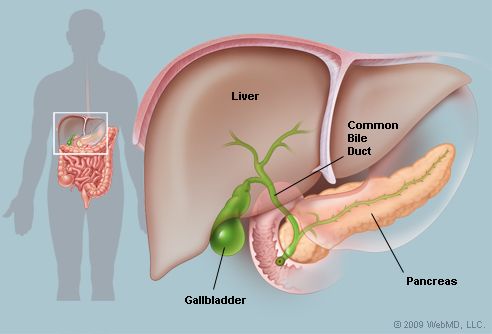
There may be no symptoms for a long period of time in the process of gall stone formation. Symptoms tend to only occur, if there is obstruction of bile flow against a stone that is migrating through the narrow cystic duct or if a stone gets caught in the narrow passage just before it comes to the ampulla of Vater at the insertion into the duodenum (for bile duct anatomy see this image).There is another passage problem between these two points, namely when the common bile duct goes through the pancreatic tissue. However, there is a lot of variation from person to person, as in some people the common bile duct does not run through the pancreatic tissue.

Cholelithiasis
Another reason for symptoms from gall stones is, when infection or inflammation sets in. This can also lead to obstruction to the cystic duct and produce identical symptoms of colicky pain.
Specific gallbladder symptoms
There might be a couple of weeks or months of non-specific symptoms following fatty meals, where right upper abdominal pain as well as fullness, belching and bloating occurs transiently. On some days it may occur, but on others it may not. Finally there is the big full blown attack where colicky pain (biliary colic) is present for several hours, perhaps even leads to a period of hospital stay where tests are performed. Pain is usually in the mid upper abdomen (epigastric area) as well as deep in the right upper abdomen and radiates into the right lower shoulder blade. The gallbladder colic is not like labor pain, but rather is a steady progressively increasing pain, which then reaches a plateau and then slowly decreases and disappears. This process lasts up to about several hours. Mostly there is no fever associated with this unless infection is part of the process.
Diagnosis
The main test for depicting stones (in medical circles known as “calculi”-has nothing to do with mathematics) is the ultrasound test. This has a high accuracy and will show stones and the size of bile ducts. It has replaced the older oral cholecystography, an X ray study, which was the common test years ago. When it comes to documenting bile duct tumors, this latter test is still being done. Once stones are detected, the clinician has to attempt to judge the clinical relevance of these findings.

Cholelithiasis (Ultrasound Exam)
The “gallbladder flush” that does not work
You may have heard about a theory that one could “flush out” gallbladder stones with a “gallbladder flush”. People swallow a mixture of olive oil and lemon juice or some other concoction and observe their stools for the next few days for roundish structures that are interpreted to be gallstones that passed the natural way.
One of my patients with gallstones
One of my patients was convinced that she had passed all her gall stones in that way and that she did not need the gallbladder surgery that I had suggested. I asked her what it would take to convince her to have the surgery. She said first a repeat ultrasound study that would prove that her gallstones were still there; secondly another gallbladder attack to convince her that she was not cured from the stones. The repeat ultrasound was identical to the first one. A few weeks later she had another gallbladder attack that precipitated a hospital admission. Needless to say that she had her gallbladder surgery shortly after, which cured her of her problem.
Fecaliths can mimic gallstones
What was she passing in the stool, which looked to her like gallstones? The answer is “fecaliths”, old stool pebbles that resemble gallstones. They get caught in some pockets of the colon until they are freed by such a concoction or simply by chance.
The human need for magic and myths in medicine is centuries old and will live on despite computers and advances in technology.
Treatment
Just because gallstones are present, does not mean that they are clinically relevant. The statistics show (see Ref. 4) that gall bladder surgery (laparoscopic cholecystectomy) has only a 0.1% mortality rate in younger patients. However, in patients older than 60 years the mortality rate goes up to 2% to 10%. Analysis of the risks of subgroups showed that among young patients who had no symptoms the mortality rate was lowest. If the patients were symptomatic, the risk was 3-fold. For asymptomatic, but older than 60 years olds, the risk was about 3 fold. Patients who were older than 60 years and symptomatic, the risk was 10-fold.
Asymptomatic patients with gallstones
Another useful statistic to keep in mind is that out of a group of asymptomatic patients with documented gall stones there is a cumulative chance of about 2% per year that they will develop symptoms (Ref. 5). Most surgeons then develop a clinical practice based on these observations that only symptomatic patients get a cholecystectomy done, but only when the acute symptoms have subsided (between gallbladder attacks).
Choledocholithiasis (gallstones in common bile duct)
Even when the gallbladder is removed, there can be new stones that form in the bile ducts. This can be a potentially very dangerous situation as the stones can get infected leading to a local infection of the common bile duct (called “cholangitis”). It is dangerous as it can lead to a systemic serious infection (sepsis). Other complications are pancreatitis and chronic liver disease. Bile is feeding any infection such as gram negative bacteria and for this reason the surgeon will want to do an early endoscopic or surgical decompression after antibiotic therapy has been initiated. Usually after this procedure there is a swift recovery.
References
1. M Frevel Aliment Pharmacol Ther 2000 Sep (9): 1151-1157.
2. M Candelli et al. Panminerva Med 2000 Mar 42(1): 55-59.
3. LA Thomas et al. Gastroenterology 2000 Sep 119(3): 806-815.
4. R Tritapepe et al. Panminerva Med 1999 Sep 41(3): 243-246.
5. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapters 20,23, 26.
6. EJ Simchuk et al. Am J Surg 2000 May 179(5):352-355.
7. G Uomo et al. Ann Ital Chir 2000 Jan/Feb 71(1): 17-21.
8. PG Lankisch et al. Int J Pancreatol 1999 Dec 26(3): 131-136.
9. HB Cook et al. J Gastroenterol Hepatol 2000 Sep 15(9): 1032-1036.
10. W Dickey et al. Am J Gastroenterol 2000 March 95(3): 712-714.
11. M Hummel et al. Diabetologia 2000 Aug 43(8): 1005-1011.
12. DG Bowen et al. Dig Dis Sci 2000 Sep 45(9):1810-1813.
13. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999.Chapter 31, page 311.
14. O Punyabati et al. Indian J Gastroenterol 2000 Jul/Sep 19(3):122-125.
15. S Blomhoff et al. Dig Dis Sci 2000 Jun 45(6): 1160-1165.
16. M Camilleri et al. J Am Geriatr Soc 2000 Sep 48(9):1142-1150.
More references
17. MJ Smith et al. J R Coll Physicians Lond 2000 Sep/Oct 34(5): 448-451.
18. YA Saito et al. Am J Gastroenterol 2000 Oct 95(10): 2816-2824.
19. M Camilleri Am J Med 1999 Nov 107(5A): 27S-32S.
20. CM Prather et al. Gastroenterology 2000 Mar 118(3): 463-468.
21. MJ Farthing : Baillieres Best Pract Res Clin Gastroenterol 1999 Oct 13(3): 461-471.
22. D Heresbach et al. Eur Cytokine Netw 1999 Mar 10(1): 7-15.
23. BE Sands et al. Gastroenterology 1999 Jul 117(1):58-64.
24. B Greenwood-Van Meerveld et al.Lab invest 2000 Aug 80(8):1269-1280.
25. GR Hill et al. Blood 2000 May 1;95(9): 2754-2759.
26. RB Stein et al. Drug Saf 2000 Nov 23(5):429-448.
27. JM Wagner et al. JAMA 1996 Nov 20;276 (19): 1589-1594.
28. James Chin, M.D. Control of Communicable Diseases Manual. 17th ed., American Public Health Association, 2000.
29. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 157, page1181.
30. Textbook of Primary Care Medicine, 3rd ed., Copyright © 2001 Mosby, Inc., pages 976-983: “Chapter 107 – Acute Abdomen and Common Surgical Abdominal Problems”.
31. Marx: Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th ed., Copyright © 2002 Mosby, Inc. , p. 185:”Abdominal pain”.
32. Feldman: Sleisenger & Fordtran’s Gastrointestinal and Liver Disease, 7th ed., Copyright © 2002 Elsevier, p. 71: “Chapter 4 – Abdominal Pain, Including the Acute Abdomen”.
33. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
34. Suzanne Somers: “Breakthrough” Eight Steps to Wellness– Life-altering Secrets from Today’s Cutting-edge Doctors”, Crown Publishers, 2008





{kind=link}