
Breast Cancer Staging
First of all, as in other cancers breast cancer staging is very important at the time of the diagnosis in order to assess and treat the patient with breast cancer accurately.
Secondly, If things are rushed and the staging is not done adequately mistakes are made in the therapy and the patient would be under treated resulting in premature death from overlooking bone metastases or lymph gland metastases. In addition, if treatments are overzealous because of an assumption that more cancer is present than there actually is, the effects of radiation could leave the patient with life long pain in the treated area.
Certainly, this could have been prevented. Exact staging is done using TNM, which is a cancer classification system. A simplified 4 stage classification system that has been used for a long time is presented here.
Breast cancer spread (staging)
Stage:
I : tumor size of less than 2 cm (= ¾”)
II : tumor size 2cm to 5 cm (= ¾” to 2″)
III : tumor size more than 5cm(=2″) with multiple positive lymph glands in axilla
IV : tumor extends to chest wall or skin and distant metastases are present
Survival data show that apart from the absence or presence of cancer tissue in the axillary glands, the clinical pathology (findings by the pathologist of breast cancer biopsies) also has a bearing on survival rates. For instance, a well-differentiated glandular breast cancer has a much better prognosis than a poorly differentiated rapidly dividing breast cancer. Likewise, the presence of estrogen receptors on the cell surface of the cancer cell will lead to better cancer survival rates. Likewise, the physician may order Tamoxifen to suppress any remaining cancer cell growth in the body.
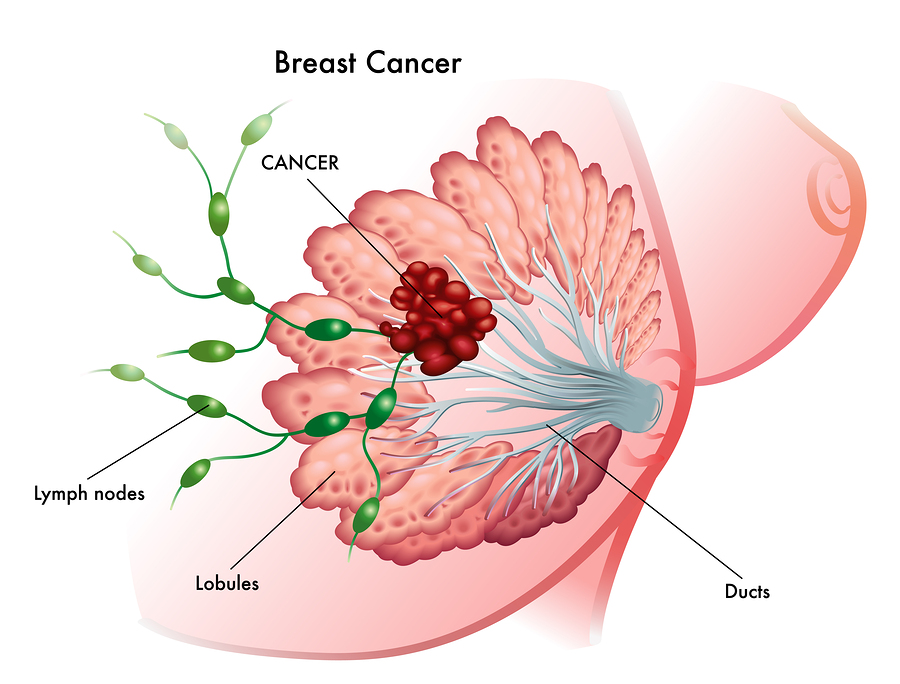
Breast Cancer Staging (Spread Of Tumor Cells Into Lymph Nodes)
Even better than Tamoxifen, bio-identical progesterone can block breast cancer cells that carry estrogen receptors on their cell surface from multiplying. Progesterone is a hormone known to the body; it has no side-effects when the person uses biological doses. The physician determines the progesterone level by saliva hormone tests (Ref.8 and 9).
Here are some survival data (Ref. 1 and 3):
5-year survival for breast cancer
| Breast cancer stage at time of diagnosis: | 5-year survival: |
| I and II | 92% |
| IIIA | 72% |
| IIIB | 38% |
| IV | 19% |
References
I used the following references apart from my own clinical experience:
1. Cancer: Principles &Practice of Oncology, 4th edition, by V.T. De Vita,Jr.,et. al J.B. LippincottCo.,Philadelphia, 1993.Vol.2: Chapter 48.
2. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 177.
3. Cancer: Principles&Practice of Oncology. 5th edition, volume 1. Edited by Vincent T. DeVita, Jr. et al. Lippincott-Raven Publ., Philadelphia,PA, 1997. Chapter 36: 1541-1616.
4. BS Herbert et al. Breast Cancer Res 2001;3(3):146-149.
5. BS Herbert et al. J Natl Cancer Inst 2001 Jan 3;93(1):39-45.
6. Conn’s Current Therapy 2004, 56th ed., Copyright © 2004 Elsevier
7. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc
8. Dr. John R. Lee and Virginia Hopkins: “Hormone Balance Made Simple – The Essential How-to Guide to Symptoms, Dosage, Timing, and More”. Wellness Central, NY, 2006
9. Dr. John R. Lee, David Zava and Virginia Hopkins: “What your doctor may not tell you about breast cancer – How hormone balance can help save your life”, Wellness Central, Hachette Book Group USA, 2005. Page 29 – 38 (Chapter 2): Risk factors for breast cancer. Page 360 to 374 explains about xenohormones and how they cause estrogen dominance. Pages 221 to 234 (chapter 12) explains that Tamoxifen is not recommendable, but that bio-identical progesterone is more powerful in preventing breast and uterine cancer.




