
Introduction
A pregnancy outside the womb is called an ectopic pregnancy, which is also known as “tubal pregnancy”.
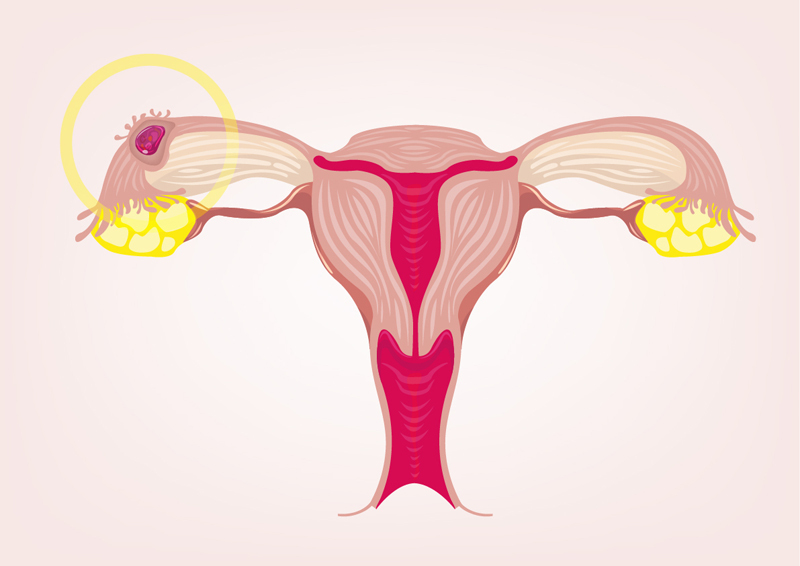
Most of these pregnancies outside the uterus develop in the upper part of the fallopian tube on either side and would then be called tubal pregnancy, but rarely it can also develop in the cervix, the ovary or in the abdominal cavity. About 1 in 100 or 200 pregnancies are ectopic (meaning “out of place”).
Previous fallopian tube infection predisposes to a tubal pregnancy, because scarring of the fallopian tube from a prior infection interferes with the normal migration of the egg from the ovary to the uterine cavity. If the egg gets stalled in between on its journey or migrates too far (cervix), an ectopic pregnancy results.
Why is this important? If it goes undetected, there will be an ectopic pregnancy rupture 12 to 16 weeks from the first day of the last period and about 1 in 800 women with a tubal pregnancy in the U.S. still die from this event despite the best possible care. This is because the blood vessels are so huge and engorged from the pregnancy (this is normal), that when it ruptures, there is an enormous amount of blood lost through abdominal bleeding, which very quickly leads to circulatory collapse and hemorrhagic shock. This in turn is very difficult to treat when the ambulance arrives at the hospital.
Symptoms of tubal pregnancy
Spotting could be one of the first symptoms associated with abdominal pain and cramping on the side where the fallopian tube pregnancy is located. These type of symptoms should prompt the woman to seek advice from her physician or gynecologist. A blood test for human choriogonadotropin would tell whether or not the levels are normal, usually the level is less in a tubal pregnancy. The gynecologist or family doctor will also order an abdominal ultrasound to document that there is a mass outside of the uterine cavity, which makes the diagnosis very likely. A laparoscopy surgery by the gynecologist will confirm the diagnosis.
Ectopic Pregnancy
Ectopic Pregnancy Treatment
The sooner the tubal pregnancy can be spotted, the better.If it is less than 3.5 cm (= 1.4″ ) in diameter, and there is no fetal heart activity on ultrasound, medical treatment with methotrexate can be attempted. However, about 25% of these cases still need surgical intervention, as this method is not always successful. With any method of removing the tubal pregnancy, it is important to monitor that all of the placental tissue is removed, as there is a danger that retained placental tissue would develop into a cancerous condition called choriocarcinoma.
This is checked in this high risk setting by doing serial blood tests of a marker called human chorionic gonadotropin, a hormone produced by placental tissue. The surgical technique today is markedly different from the past. In the past the tubal pregnancy was excised with all of the tube on the affected side. However, there was only one tube left and the likelihood of a normal pregnancy was significantly reduced. Today a tube preserving technique is used, where the pregnancy and placenta are removed and then careful reconstructive surgery is done, if necessary using an operative microscope. This way a normal pregnancy can often take place when the affected tube has been reopened through surgical means. Future pregnancies are followed with serial ultrasonic tests.
References:
1. DM Thompson: The 46th Annual St. Paul’s Hospital CME Conference for Primary Physicians, Nov. 14-17, 2000, Vancouver/B.C./Canada
2. C Ritenbaugh Curr Oncol Rep 2000 May 2(3): 225-233.
3. PA Totten et al. J Infect Dis 2001 Jan 183(2): 269-276.
4. M Ohkawa et al. Br J Urol 1993 Dec 72(6):918-921.
5. Textbook of Primary Care Medicine, 3rd ed., Copyright © 2001 Mosby, Inc., pages 976-983: “Chapter 107 – Acute Abdomen and Common Surgical Abdominal Problems”.
6. Marx: Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th ed., Copyright © 2002 Mosby, Inc. , p. 185:”Abdominal pain”.
7. Feldman: Sleisenger & Fordtran’s Gastrointestinal and Liver Disease, 7th ed., Copyright © 2002 Elsevier, p. 71: “Chapter 4 – Abdominal Pain, Including the Acute Abdomen”.
8. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc




