
Introduction
Sources for beef tapeworm (also known as Taenia saginata) are raw or undercooked beef, if it contains a cysticercus.
This is a small cyst that contains a live scolex, a head of the beef tapeworm. When a human ingests this with the raw meat, it hooks onto the inside of the intestinal wall. From there the tape worm matures by growing the neck and the proglottides (=segments) that contain the hermaphroditic sex organs, and the pregnant, egg containing uterus (see life cycle image, thanks to www.stanford.edu for this image)
The last segment is always shed while the other end grows so that the overall length stays about the same for years (about 2 to 3 feet) unless the patient gets treated. This infection is uncommon in the U.S. as federal inspectors monitor the cattle. However, in Mexico, South America, Africa, the Middle East, and Eastern Europe it is common in cattle.
Signs and symptoms
Unexplained weight loss may be the only sign that the patient has a beef tapeworm. If the patient is observant, and a whitish segment that moves slightly is found in the stool, the doctor can order to have this analyzed in a laboratory. Sometimes the patient has abdominal pain and diarrhea.
Diagnostic tests
Feces can be examined for eggs from ruptured segments or the gravid segments filled with eggs can be seen. A clear, self adhesive tape can be used to obtain egg samples from skin around the anal area, which reveals the eggs under the microscope.
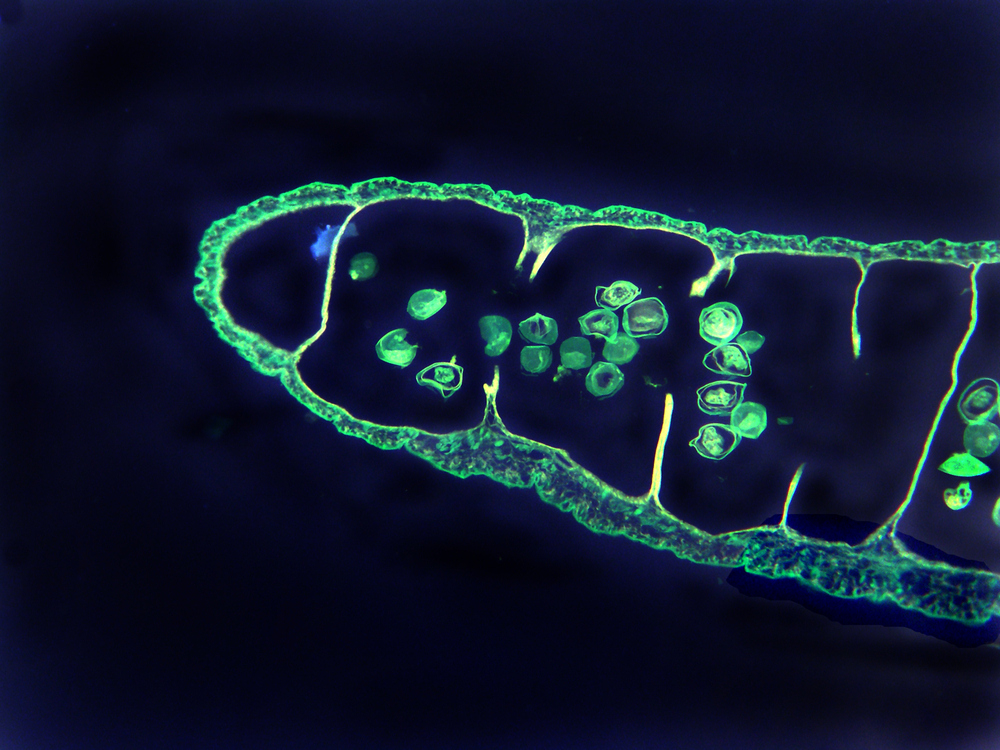
Beef Tapeworm (End Piece With Sac Of Eggs)
Health alert
____________________________
Beef tape worm infestation can be prevented by cooking beef at 56°C (=133°F) for 5 minutes; refuse to eat tartare (raw beef)!
____________________________
Treatment
A single dose of praziquantel (brand name: Biltricide) is effective. Alternatively niclosamide can be given as a one dose treatment. Either of these drugs allows the patient to pass a dead tapeworm in 90% of all cases.
References:
1. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 161.
2. TC Dixon et al. N Engl J Med 1999 Sep 9;341(11):815-826.
3. F Charatan BMJ 2000 Oct 21;321(7267):980.
4. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 43.
5. JR Zunt and CM Marra Neurol Clinics Vol.17, No.4,1999: 675-689.
6. The Merck Manual, 7th edition, by M. H. Beers et al., Whitehouse Station, N.J., 1999. Chapter 162.
7. LE Chapman : Antivir Ther 1999; 4(4): 211-19.
8. HW Cho: Vaccine 1999 Jun 4; 17(20-21): 2569-2575.
9. DO Freedman et al. Med Clinics N. Amer. Vol.83, No 4 (July 1999): 865-883.
10. SP Fisher-Hoch et al. J Virol 2000 Aug; 74(15): 6777-6783.
11. Mandell: Principles and Practice of Infectious Diseases, 5th ed., © 2000 Churchill Livingstone, Inc.
12. Goldman: Cecil Textbook of Medicine, 21st ed., Copyright © 2000 W. B. Saunders Company
13. PE Sax: Infect DisClinics of N America Vol.15, No 2 (June 2001): 433-455.




