
Introduction
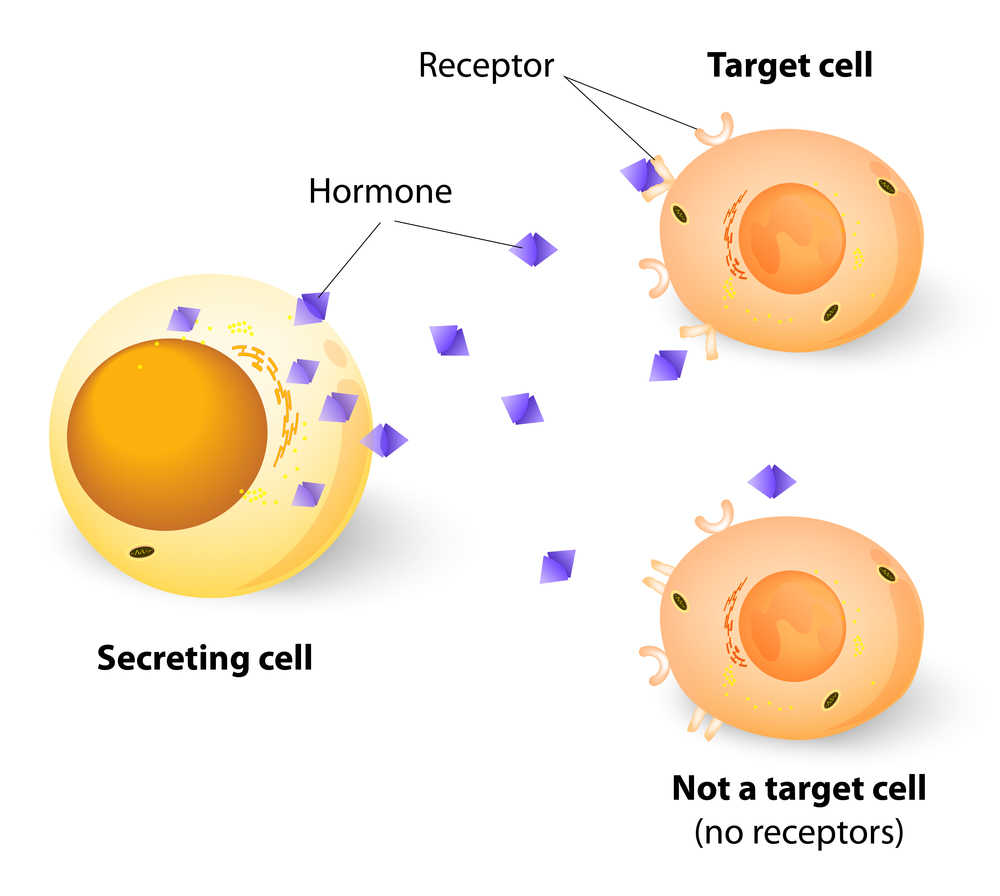
With nephrogenic diabetes insipidus the patient does a lot of urinating because of a defect of hormone receptors in the kidneys. The loss of vasopressin receptors (synonymous to antidiuretic hormone receptors or ADH receptors) at the level of the kidney tubules makes it impossible for the kidney to concentrate urine to a higher osmolality than that of plasma of the blood (also see Ref. 6) resulting in an inability to concentrate the urine within the kidneys.
This leads to ADH resistance although ADH (vasopressin) is circulating in normal concentrations in the blood. In other words the hormone key does not quite fit into the key hole (due to defective receptors).
Symptoms
The symptoms of urinating often (polyuria) and always being thirsty and drinking water (polydipsia) are common. This is combined with a diluted urine (hypotonic) and these are the only symptoms that the mother and physician can see as the baby that is born with this condition cannot communicate thirst. For the same reason it is often only when a baby suddenly has a severe neonatal seizure that the physicians start investigating. At that time it may be apparent that there is severe dehydration with high sodium (hypernatremia) in the blood.
The baby may have a fever and vomiting as well. It is important that the diagnosis of nephrogenic DI is made early by a pediatrician so that brain damage from child mental retardation can be avoided.
Diagnosis
The diagnosis in older children can be done with the water deprivation test described above. In infants the pediatrician may have to modify the testing somewhat, but osmolality testing of blood and urine are still the mainstay of diagnosis.
Nephrogenic Diabetes Insipidus
Treatment
The patient needs to have free access to adequate water intake. Otherwise the urine output can be modified with sodium restriction, the use of the diuretic thiazide or potassium sparing amiloride (brand name: Midamor) and anti-inflammatories such as indomethacin (brand name: Indocid), which is a prostaglandin inhibitor. The potassium sparing amiloride is particularly useful in cases of Lithium therapy (for bipolar disease) induced nephrogenic DI. Amiloride excretes Lithium and prevents the aldosterone release that occurs with regular diuretics such as hydrochlorothiazide. Regular diuretics would lead to sodium and lithium retention, which could lead to severe side effects (more details under Ref. 10).
Prognosis
The outlook used to be poor, but with newer medications and approaches such as mentioned above a normal life expectancy might now be possible. Close physician supervision is needed.
References
1. MT Kailasam et al. J Hypertens 2000 Nov 18(11): 1611-1620.
2. G Chinetti et al. Inflamm Res 2000 Oct 49(10): 497-505.
3. St. Paul’s 46th Annual Cont. Med. Educ. Course for Prim. Phys., Nov. 14-17, 2000. Dr. David Thompson, Div. of Endocr., Vancouver Hosp. and UBC.
4. B J Goldstein Int J Int Pract 2000 Jun 54(5): 333- 337.
5. M Maghnie et al. N Engl J Med 2000 Oct 5;343(14): 998-1007.
6. E Albertazzi et al. J Am Soc Nephrol 2000 Jun 11(6):1033-1043.
7. M Funk et al. American Journal of Emergency Medicine Vol.19,No.6, Oct.2001, W. B. Saunders Company
8. Ferri: Ferri’s Clinical Advisor: Instant Diagnosis and Treatment, 2004 ed., Copyright © 2004 Mosby, Inc.
9. Rakel: Conn’s Current Therapy 2004, 56th ed., Copyright © 2004 Elsevier
10. http://en.wikipedia.org/wiki/Nephrogenic_diabetes_insipidus




